
There are two workshops: one very short and one very long.
- Evoke Wellness.
Back in December, Council had a lot of questions for these guys. They offer mental health and addiction treatment for people referred over by the police. We’ve allocated 150K of Covid money for this. This is a follow up discussion with the director at Evoke.
Amanda: What’s it look like if you’re receiving services?
The director gives an extremely detailed answer!
- Prescreen for eligibility. Detox? Residential? Intensive Outpatient?
- Say we’re starting with detox. Then there’s an evaluation and intake process.
- Then you’re seen by nursing staff to get orders from the medical director on the detox protocol, medication regimen
- Detox lasts 5-7 days. Completely voluntary. You’re free to leave at any point.
- Residential: 21-28 days. Could be detox and then residential.
- In the residential part: first there’s a biopsych-social assessment: trauma history, drug use history, family relationships, everything. You need a full picture to treat the whole person.
- Clinical team and medical team working together to monitor the patient 24/7.
- During the day: like school, 6 hours a day. Learn about substance abuse and mental health conditions, tools, coping skills to hopefully achieve longterm sobriety.
- Breakfast, meds, 9:30-5:30 programming, community involvement with 12-step panels holding meetings with clients.
- You also get a therapist and case manager. The case manager will help with the discharge process.
- Therapist meets weekly and as needed.
- 6 hours/day of group therapy.
- Longer lengths of stay produce better outcomes. Typically 28-35 days.
- Discharge plans: typically clients take the clinical recommendation for a sit down placement in a PHP (partial hospital hospitalization) – lower level of care, higher level of freedom, and so own down the levels of care.
Amanda: How often is the intake the first time the person’s ever run through their trauma?
Answer: Depends if they’ve ever had treatment before. Could be first time, could have relapsed.
Amanda: Typical client to staff ratio?
Answer: 8:1 ratio, plus nursing staff and on-call medical director and leadership team.
Amanda: On the discharge plan: If you don’t want to go through everything, can you still get a discharge plan?
Answer: Yes. And if they won’t accept the discharge plan, our case managers will help connect them with resources that work for them.
Amanda: What about people that are indigent? How does medication work upon discharge?
Answer: For all clients, detox meds are covered for free, for 5-7 days. They are responsible for their medications, but if they have no resources, we will keep providing it. The discharge coordinator will work with them to find the community resources to stay on their medications.
Alyssa: Last year, I asked for info about Evoke. They were in the process of getting a mental health license – did that happen?
Answer: We are licensed for co-occuring disorders. There must be substance disorder with a mental health disorder. Actually pretty rare to have a substance issue without a mental health issue, so this is pretty much all our patients. We do not currently serve clients that only have a mental health issue and no substance abuse.
Alyssa: This helps San Marcos?
Chief Standridge: The goal is jail diversion. We’re using funds from both San Marcos and Hays money. If they have insurance, we use that first. If they’re indigent, we try to use our funds. But only if they’re residents of San Marcos.
Everyone is really pleased by the high quality of the answers given by the director.
Alyssa: I’m very hopeful? There’s a lot of structural root causes and obstacles that have to be overcome, and we have to think about those when it’s time to budget. And the public defenders office has been really helpful in locating resources. But I am anxious about the rise in need for support services. We’re setting people up for failure if we don’t supply resources.
Shane: I’m tickled to death! How it all came together, as a team.
(This is Covid money, so we’ll have to figure out how to fund it going forward.)
…
Workshop 2: SMPD. This is a 2 hour presentation!
This is SMPD’s opportunity to put their best foot forward. This is a description of all the trainings and guard rails in place at SMPD. Everything is couched in really positive terms – “Do we make mistakes? Sure! But we then unpack it and learn from it.”
This isn’t bad! It’s totally fine. It’s what any other department would do. However, a police department requires an extra level of skepticism, because of the sordid history leading up to this moment in time.
Usually I’d use Council questions to look for cracks in the presentation. But they ran out of time, because the council meeting starts at 6 pm.
So this is a very glowing presentation, without any opportunity to give a counter-narrative. Anyway, I’m just the messenger. Don’t shoot me.
…
Chief Standridge came here four years ago. We’re kind of summarizing the internal protocols that he’s implemented over this time.
There are five different speakers.
Speaker #1: Internal changes
“ABLE” stands for Active Bystander for Law Enforcement. This is basically like “Friends Don’t Let Friends Drive Drunk.” How do you create an environment where cops will tattle on each other?

The goal is for the consequences of not intervening to be bigger than the consequences of intervening. They do some training around interventions as well.
Here’s how many internal cases they’ve dealt with:

I mean, it’s absolutely impossible to interpret this. Is this a lot, or a little? How often are incidents going unreported? Would I agree with the outcomes if I knew all the details of the incidents?
There’s no way that PD could answer these questions! But it also means that we can’t really makes sense of this data.
It’s like if five people go to the doctor for measles, and the doctor treats three of them, and diagnoses one with allergies and one with mumps.
- That doesn’t tell you much about the number of measles cases in the rest of the town
- It also doesn’t tell you if the doctor is making correct diagnoses
Both those things would be much harder to figure out.
Here are the investigations that were found to be substantiated:
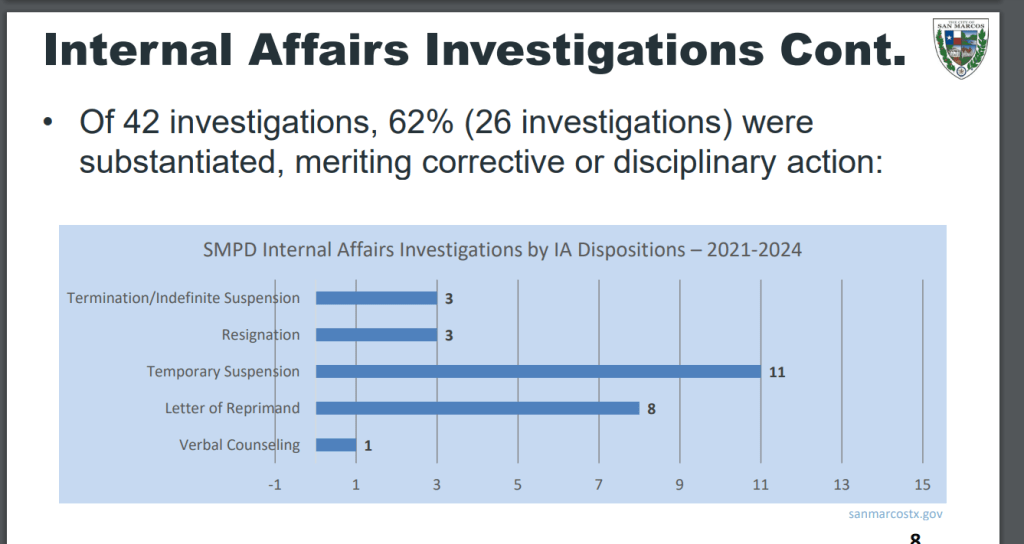
In 2021, we had one IA investigator. Now we have four. So that definitely helps have more eyes looking out for bad behavior.
…
The Event Review Board
The Event Review Board reviews every incident, use of force, pursuit, and preventable accident. They try to see what the department could change to reduce these events.
It’s a broad group of people and they’re supposed to look at any potential event, no matter how minor.

Some data:

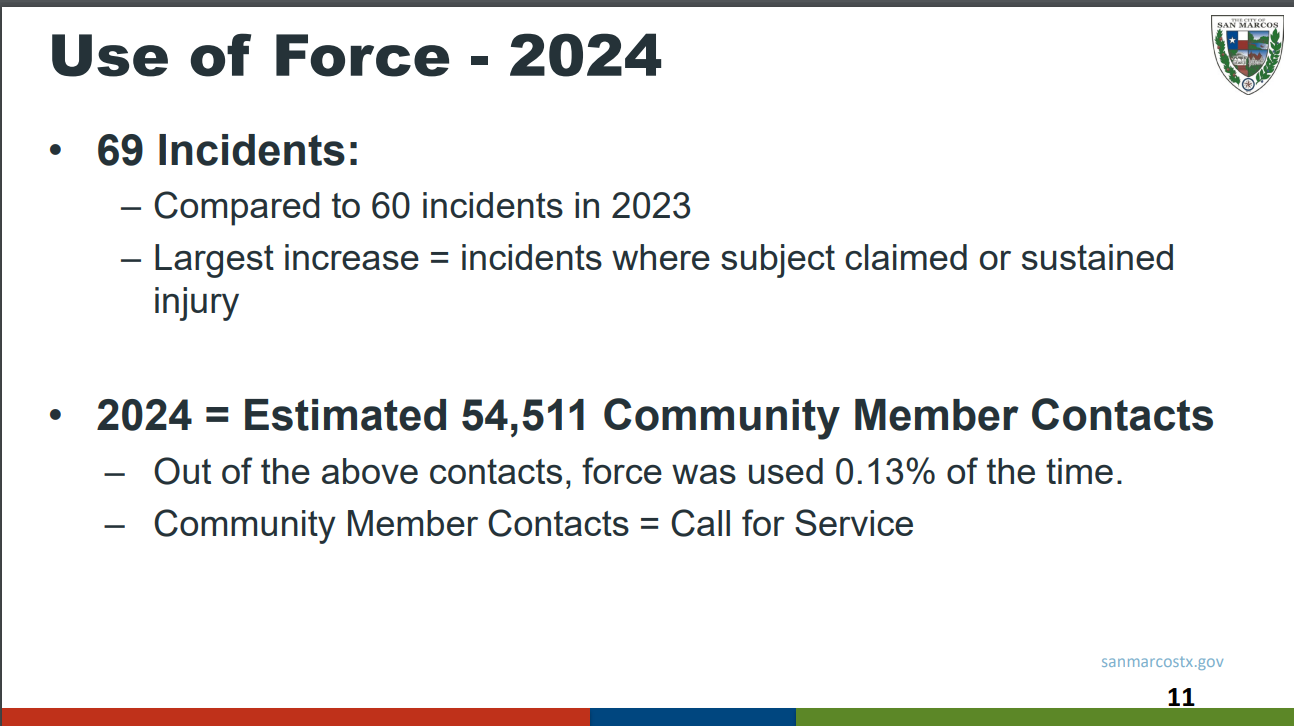
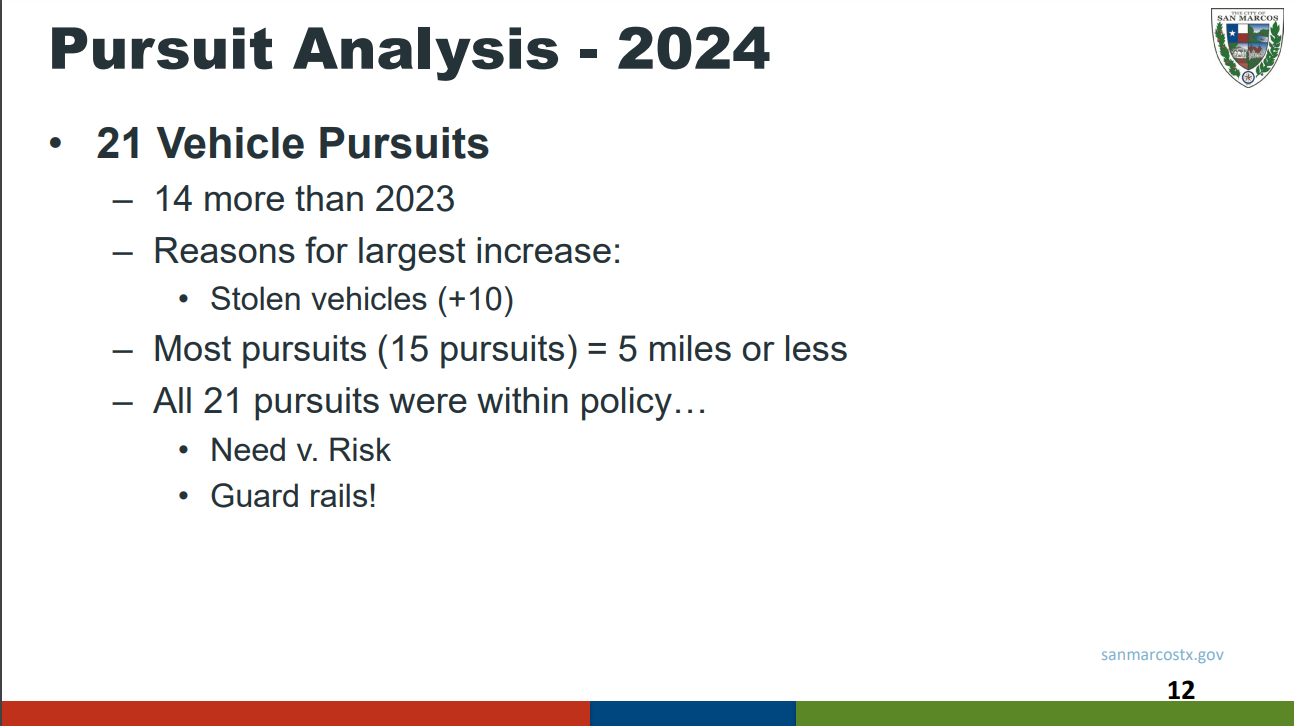

Again, I just don’t have enough context to make sense of these numbers.
The speaker might have said given good context! But this was a three hour presentation, and if she did, I didn’t jot it down in my notes.
Also:

None of these were available last April, when Malachi Williams was killed. Alyssa brings this up.
Amanda asks about the costs of these?
Taser 10: $343K for 123 officers, or about $2789 per officer, per year. (Includes the Taser 10, body cameras, unlimited video storage, training, and software licensing.)
BolaWrap: $1,299.99 each, and $38.99 each for cartridgets
40 mm foam bullet launcher thing: $1,273.50 each
I don’t know if each officer gets each thing, but that would come to $5362 per officer. With 123 officers, it’s about $660K.
Look, I want the officers to use less lethal force. I’m just pointing out that SMPD spends bigger sums of money, and they do it much more quickly and easily than any other department.
…
This next thing is actually really great.
Suppose you stop someone and they don’t speak English. You open up this Voyce app, and there’s a live translator. You pay by the minute.

Notice they can provide sign language as well. (But it only works if officers remember that people can be deaf. This would not have helped John Kelley, the deaf man that was tased in 2019 for not responding when SMPD told him to stop.)
The speaker says that there was one time that they needed a Mandarin translater at 3 am. This is pretty invaluable for that. (It was originally designed for the medical community. Seems invaluable there, too.)
This app doesn’t help you figure out what language the other person is speaking though. You have to use google or something.
That was all the first speaker!
…
Next speaker: Accreditation

So I guess not all the PDs are accredited, but now we are?
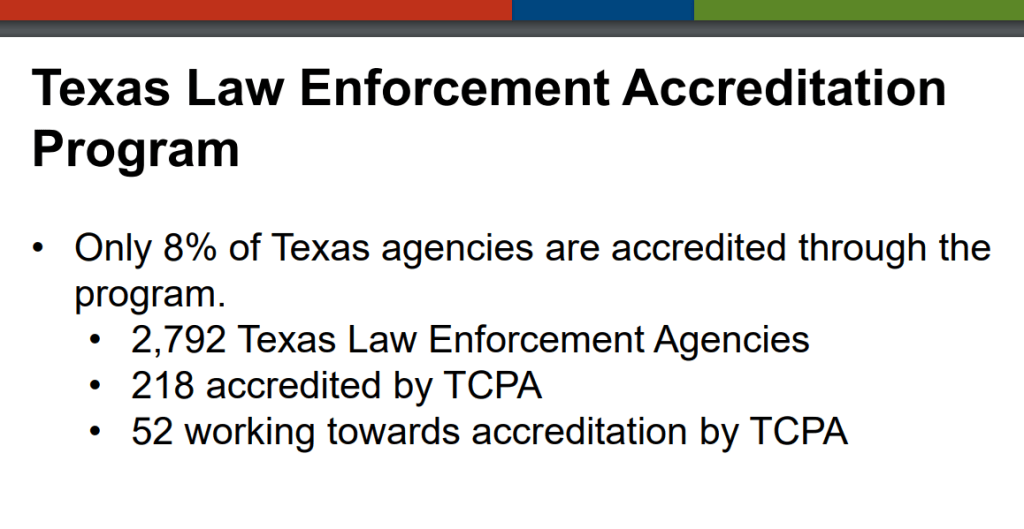
We’re not there yet, but we’re working towards it.
Basically you have to come up with policies that satisfy the agency in these areas:

You have to show compliance with 173 best practices.
(This meeting was the day when it was super windy and there was all the spooky smoke and dust hanging over the city. Everyone’s alarms kept going off for the evacuations up in Kyle.)
Anyway, it sounds like it’s a ton of work:

And then you have to stay accredited:
…
Onto the next speaker!
This one is super interesting – it’s on our 911 call center.

Basically, there’s a nationwide shortage of 911 dispatchers. We used to have 9 vacancies. We filled over half of them, and we’ve got a current batch of highers to fill the rest.
What happened is that we started paying a reasonable salary, and got a reputation as a good place to work. So we’re in a much healthier spot now.

911 callers also have language barriers. Instead of the VOYCE app, they use something called CyraCom:

Alyssa points out that this happened in the original 911 call involving Malachi Williams. The caller only spoke Spanish. While they were connecting with CyraCom, there was just this awful dead silence, where the caller had no idea whether or not they were going to get any help.
Alyssa suggests having a few pre-scripted lines like, “One moment while we connect with a translator” or something. This is a great idea.
We’re also trying a new program:
This is a program where they transfer mental health calls out to trained mental health providers, who will connect the person with local resources, or stay on the line and talk the person through whatever’s going on.
They can also transfer the call back to 911, if they think we need to send out an emergency response, after all. The responder then goes right out, because the call is already in the system.
They’ve been doing it since November. It turns out that most of the calls do come back to us, after all? And we end up sending someone out. It’s a work in progress!
…
Next speaker! The SMPD Mental Health Unit.

I don’t know what the training to be a Mental Health Officer really means. Is it a course? Is it multiple courses? Is it like a Master’s degree? Are you supervised by a mental health professional?
(I’m sure I could look it up, but I’m just trying to first get this whole entry out on time.)
It sounds like they do good things: they sit with people who are scared and nervous before testifying or going to court. They get food boxes from Hays County Food Bank if someone needs it. They’re generally problem-solving and checking in on people’s well-being. They will sometimes stay with someone for months, making regular follow ups to help manage someone’s care.
Here, have some data:

An “emergency detainment” is if someone is an immediate danger to themselves of others. They try to avoid doing that, though. It may mean taking them to an ER or a substance abuse facility. (But not jail.)
…
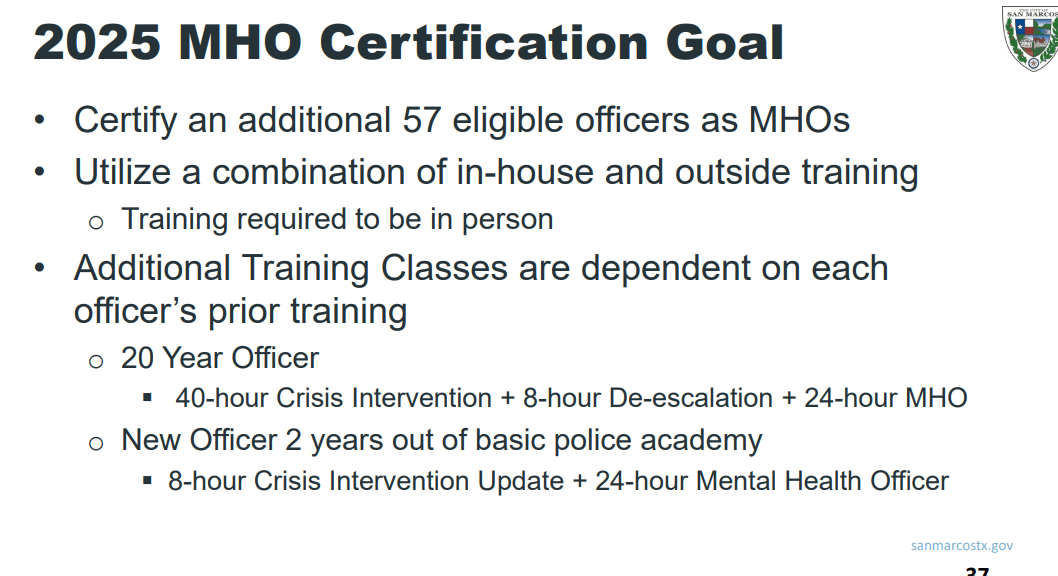
Next speaker! What comes next with Mental Health Officers?
Here’s what the state is doing:
It used to be that officers had two options:
- Take someone to an emergency room
- Take someone to jail and go through courts.
Now we’ve got more options. The state created a big Mental Health Officer framework in 2015.
Here’s what we’ve got so far:

Here’s what we’re aiming for:
…
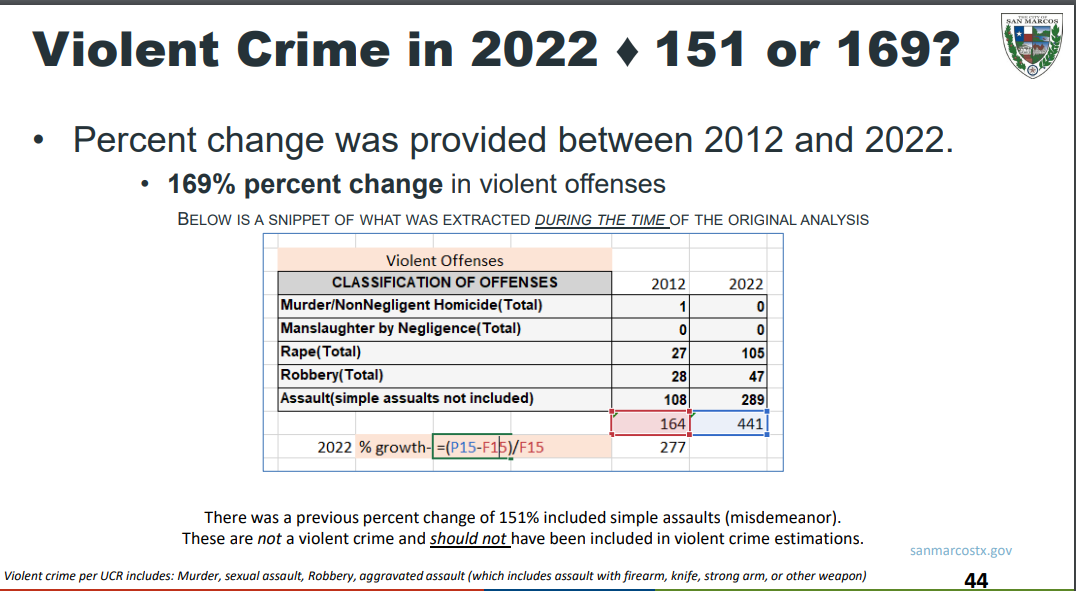
Next speaker! Context of Crime.
We report crime in two ways:

We are transitioned in 2018/2019 from UCR to NIBRS, which is better data. But any longterm comparison requires UCR data.
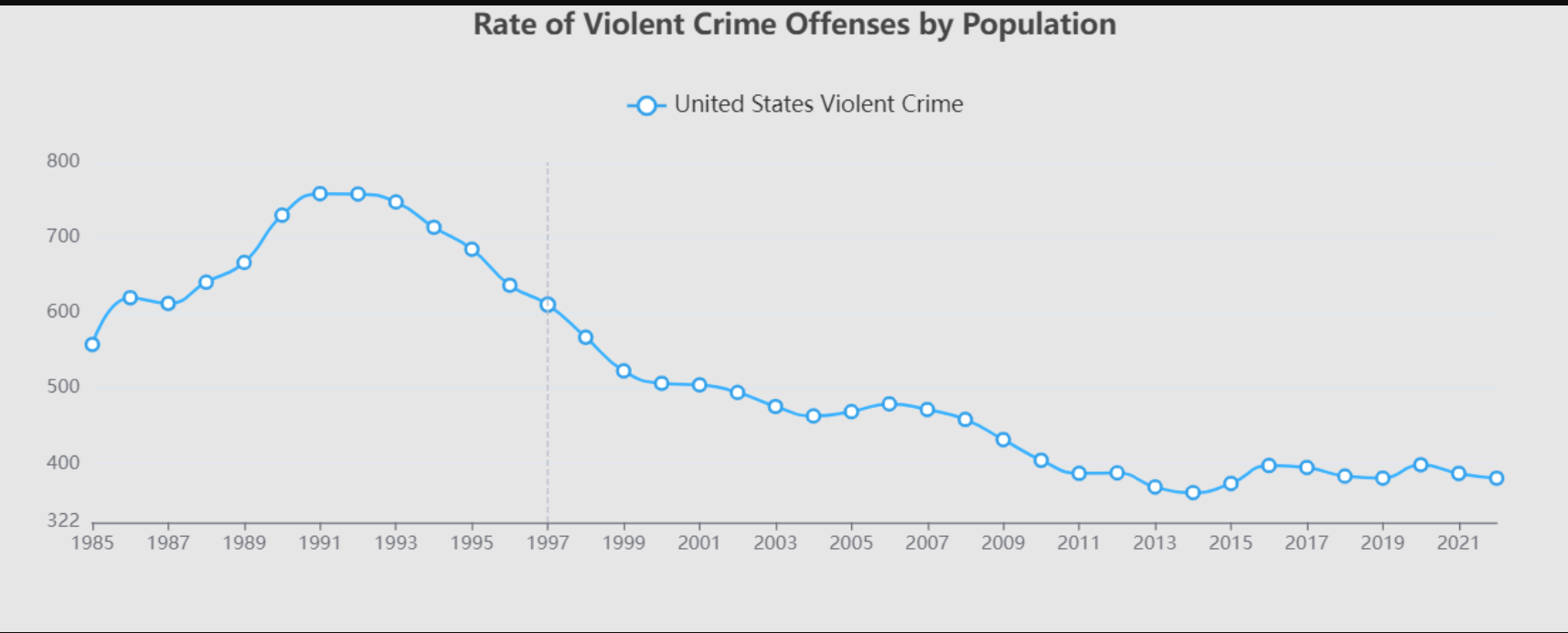
Longterm violent crime:
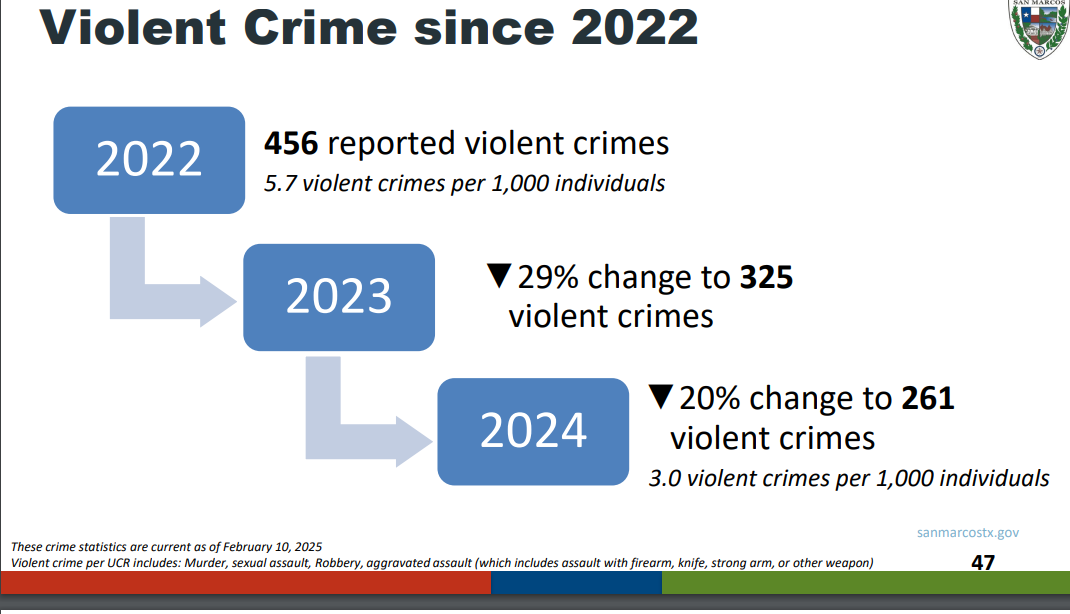
Short term crime rates:

Note from me: On the motor vehicle theft, this is happening everywhere:

But it’s always worth remembering that crime is way down, overall:

…
Back to the presentation.
More crime trends:

and specifically violent crimes:
Saul asks a great question – does this include Texas State data?
Answer: No. They have their own police and their data is not included.
Again, this is mostly just following national trend lines, as the nation returns to baseline after Covid:

It’s still a good thing!
And it’s still way, way lower than 30 years ago:
This recent data also corresponds time-wise with Chief Standridge arriving in 2021. So we are simultaneously implementing new strategies:
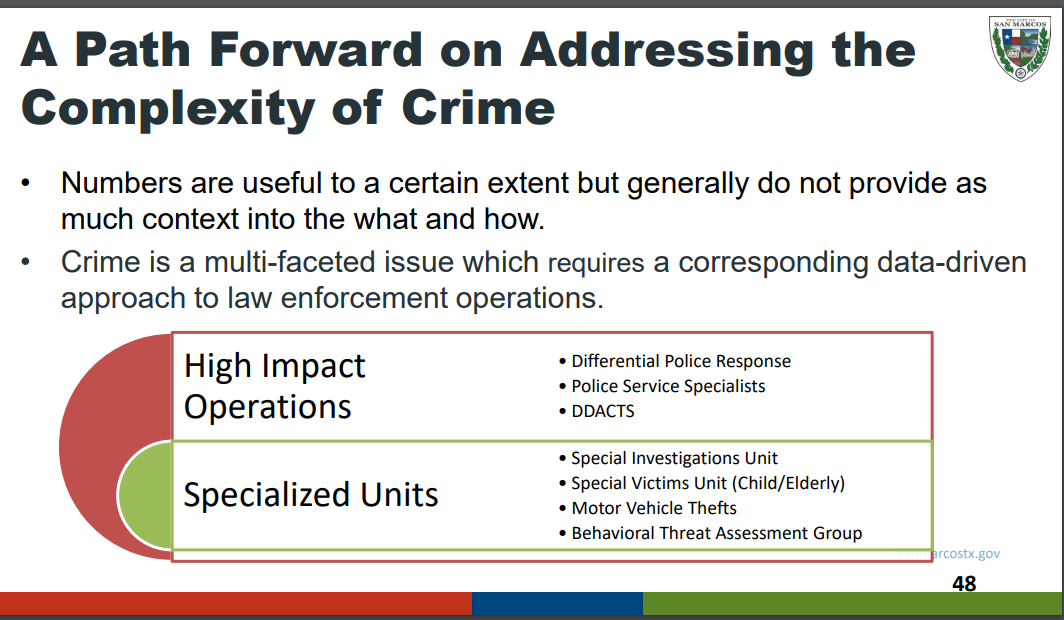
There’s a special victims unit:

They partner with Hays-Caldwell Women’s Shelter.
…
Next up is Chief Standridge! He is very apologetic.
There is a specific Chief’s Advisory Panel. In order to get community feedback, they drew up some questions about the public’s crime-related fears.
The plan was for everyone on the panel to chat up their neighbor and get some informal feedback. Max Baker offered to digitize the survey and share it with the San Marcos Civics Club.
When staff got the responses, they threw out anything that didn’t seem relevant to the question at hand. Chief Standridge is extremely apologetic to this. He apologizes profusely and specifically to Max and the public.
Here are the remaining answers:
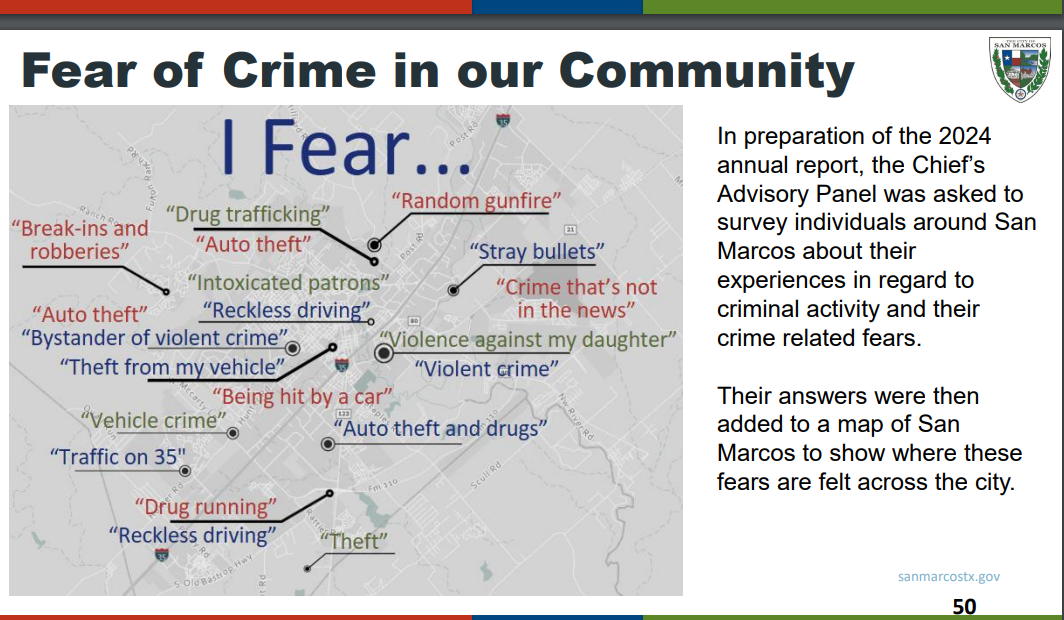
He promises to get the full data, including the extra answers, out as quickly as possible.
(My personal answer is car crashes on I-35. That terrifies me.)
…
By this point, it is 5:30, and the looming 6 pm meeting starts to take over the presentation.
Councilmembers have lots of questions, but there’s not really time for them.
…
Next presentation! School Resource Officers.

SROs are supposed to be three things: Counselor, educator, and law enforcement:

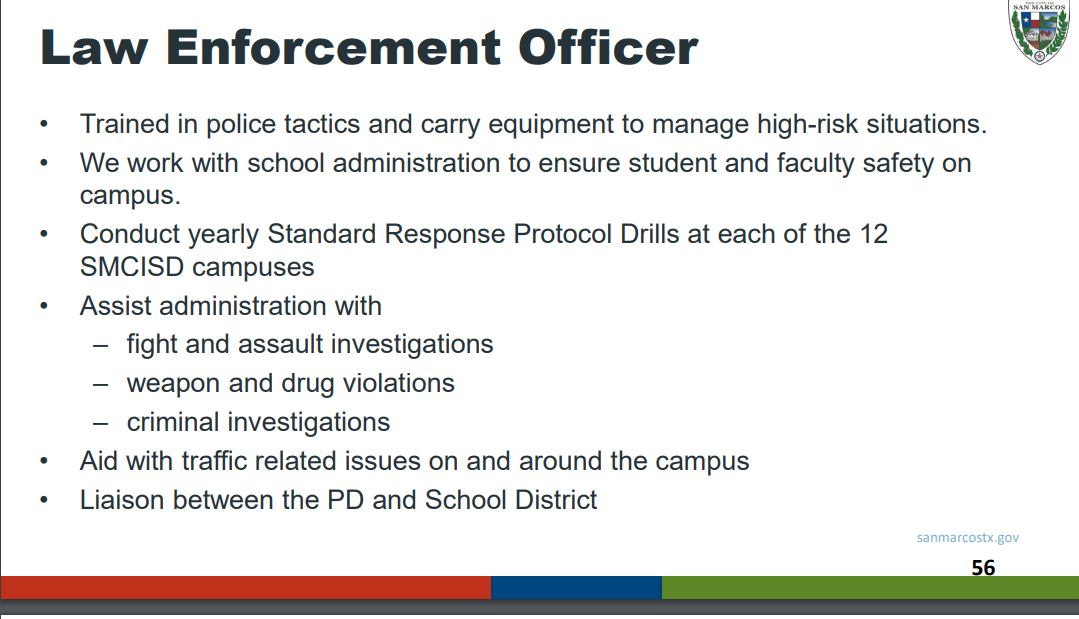
But not these things:

We have five total:

We’ve been doing this since Columbine, and most of the community is pretty happy with it:

…
Back to Chief Standridge:
He sums up with this program for the next year:

At this point, they are almost out of time. There are slides on the Marijuana Decriminalization Dashboard, but he doesn’t get to them. But it’s all publicly available here.
The full slide show is also available here.
…
There’s a very quick Q&A, but it’s rushed and haphazard. Hopefully there will be a real Q&A scheduled in the future.
Holy moly, that was long.









.png){kind=link}